- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
All you need to know about the female orgasm

A very good video illustrating the Interrupted Sub-Dermal Sutures
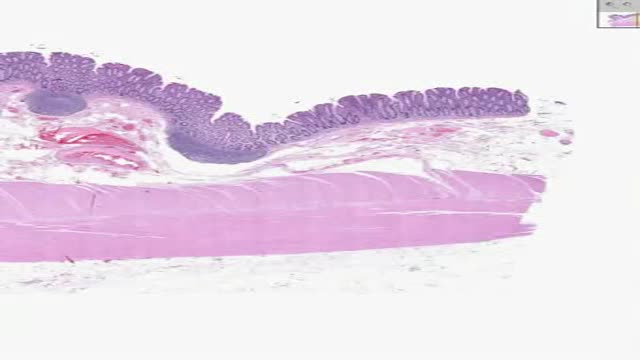
Histology of Colon

Thoracentesis is used diagnostically to establish the cause of a pleural effusion. It can also be performed to drain large effusions that lead to respiratory compromise
Try our MULTIPLE CHOICE QUESTIONS and WATCH MORE VIDEOS at www.boxmedicine.com!
Inguinal and femoral hernias need not be confusing. In this tutorial you will be presented with colourful diagrams and animations to cover important areas, such as the anatomy of what goes on in these two conditions, the examination of groin hernias and a simple explanation of the difference between incarceration, strangulation and obstruction, in and amongst a systematic look at the clinical topic. More tutorials at www.boxmedicine.com.

Dependent Personality Disorder Information

Sialadenitis is an infection of the salivary glands. It is usually caused by a virus or bacteria . The parotid (in front of the ear) and submandibular (under the chin) glands are most commonly affected. Sialadenitis may be associated with pain, tenderness, redness, and gradual, localized swelling of the affected area.

A bulla is a fluid-filled sac or lesion that appears when fluid is trapped under a thin layer of your skin. It’s a type of blister. Bullae (pronounced as “bully”) is the plural word for bulla. To be classified as a bulla, the blister must be larger than 0.5 centimeters (5 millimeters) in diameter. Smaller blisters are called vesicles.
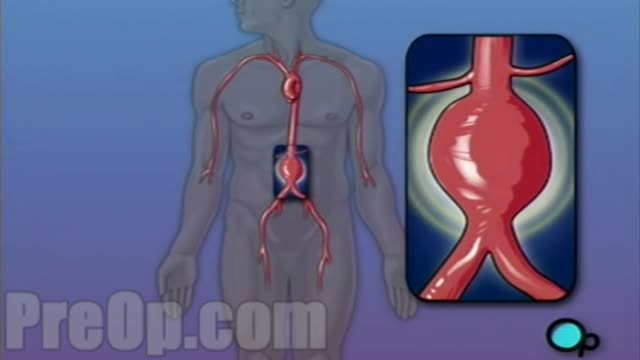
For this surgery, your doctor makes a large incision in the abdomen to expose the aorta. Once he or she has opened the abdomen, a graft can be used to repair the aneurysm. Open repair remains the standard procedure for an abdominal aortic aneurysm repair. Endovascular aneurysm repair (EVAR).

Massive bone defects (>8 cm) will not unite without an additional intervention. They require a predictable, durable, and efficient method to regrow bone. The Ilizarov method of tension stress, or distraction osteogenesis, first involves a low-energy osteotomy1 - 5. The bone segments are then pulled apart, most often using an external device at a specific rate and rhythm (distraction phase), after which the newly formed bone (the regenerate) requires time for consolidation. The consolidation phase is variable and usually requires a substantially greater amount of time before the external device can be removed. Our technique of tibial bone transport over an intramedullary nail using cable and pulleys combines internal and external fixation, allowing the external fixator to be removed at the end of the distraction phase. This increases the efficiency of limb reconstruction and decreases the external-fixator-associated complications.
Peptic Ulcer 3D

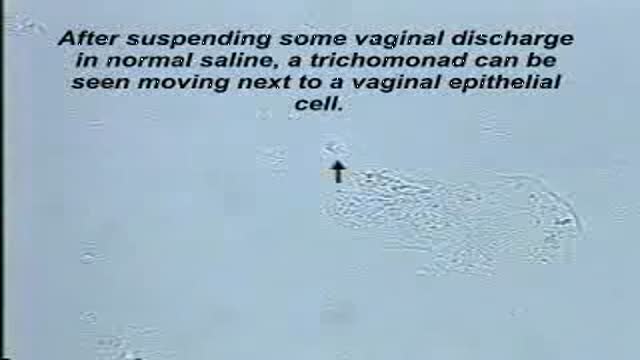
Trichomonas is best seen on the Normal Saline slide.These protozoans are about the same size as a white blood cell (a little smaller than a vaginal epithelial cell), but their violent motion is striking and unmistakable.
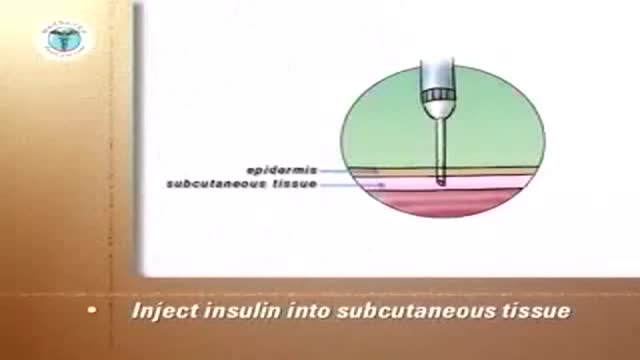
Insulin Pen

Indications for endovascular repair of the iliac artery are: Stenosis or (short-segment) occlusion of iliac artery (TASC type A and B, TASC C lesions are controversial) with ipsilateral lower extremity ischemia (lifestyle-limiting, progressive claudication, rest pain, gangrene). Patients with asymptomatic aneurysm greater than 4 cm in diameter. An iliac aneurysm which has also increased in size by 0.5 cm in last six months. Symptomatic iliac artery aneurysms mandate endovascular (or open) repair regardless of size. Patients with long occluded lesions/poor run-off/acute limb ischemia are poor endovascular candidates.

Emergency contraception is a method of birth control you can use if you had sex without using birth control or if your birth control method did not work correctly. You must use emergency contraception as soon as possible after unprotected sex. Emergency contraception pills are different from the abortion pill. If you are already pregnant, emergency contraception pills do not stop or harm your pregnancy. Emergency contraception has also been called the "morning-after pill," but you do not need to wait until the morning after unprotected sex to take it. Emergency contraception is not meant to be used for regular birth control. Talk to your doctor or nurse about regular birth control to help prevent pregnancy. Nearly half of all pregnancies in the United States are unplanned.1

open multi puncture testicular biopsy to retrieve sperm for ICSI (IntaCytoplasmic Sperm Injection) Procedure video

Bipolar disorder, formerly called manic depression, is a mental health condition that causes extreme mood swings that include emotional highs (mania or hypomania) and lows (depression). When you become depressed, you may feel sad or hopeless and lose interest or pleasure in most activities. When your mood shifts to mania or hypomania (less extreme than mania), you may feel euphoric, full of energy or unusually irritable. These mood swings can affect sleep, energy, activity, judgment, behavior and the ability to think clearly. Episodes of mood swings may occur rarely or multiple times a year. While most people will experience some emotional symptoms between episodes, some may not experience any. Although bipolar disorder is a lifelong condition, you can manage your mood swings and other symptoms by following a treatment plan. In most cases, bipolar disorder is treated with medications and psychological counseling (psychotherapy).

Unique 3D technology from Olympus:
http://www.olympus-europa.com/....medical/en/medical_s
Discover the 3rd dimension of endoscopy and experience laparoscopy in a totally new dimension.
Contact us for more information:http://www.olympus-europa.com/....medical/en/medical_s

Many over-the-counter medications can help relieve heartburn. The options include: Antacids, which help neutralize stomach acid. Antacids may provide quick relief. But they can't heal an esophagus damaged by stomach acid. H-2-receptor antagonists (H2RAs), which can reduce stomach acid. H2RAs don't act as quickly as antacids, but may provide longer relief. Proton pump inhibitors, such as lansoprazole (Prevacid 24HR) and omeprazole (Prilosec OTC), which also can reduce stomach acid.
