- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Bipolar disorder, formerly called manic depression, is a mental health condition that causes extreme mood swings that include emotional highs (mania or hypomania) and lows (depression). When you become depressed, you may feel sad or hopeless and lose interest or pleasure in most activities. When your mood shifts to mania or hypomania (less extreme than mania), you may feel euphoric, full of energy or unusually irritable. These mood swings can affect sleep, energy, activity, judgment, behavior and the ability to think clearly. Episodes of mood swings may occur rarely or multiple times a year. While most people will experience some emotional symptoms between episodes, some may not experience any. Although bipolar disorder is a lifelong condition, you can manage your mood swings and other symptoms by following a treatment plan. In most cases, bipolar disorder is treated with medications and psychological counseling (psychotherapy).

Here Drs Oetting and Shriver of the University of Iowa demonstrate the McCannel technique of fixing an IOL to the iris. In this video both the standard McCannel suture retrieval technique and the Siepser/Chang modifed technique are demonstrated. A 10-O prolene with a long curved ctc-6 needle is u...sed to place a suture through the iris and under an 3 piece IOL haptic. Using the standard technique the two ends of the suture are retrieved through a common paracentesis near the fixation site and tied externally. The other haptic is tied using the Siepser sliding knot technique as described by Chang for this indication with an internal knot. The standard technique is a bit easier but does not allow as thight a knot for fixation of the iris to the haptic.
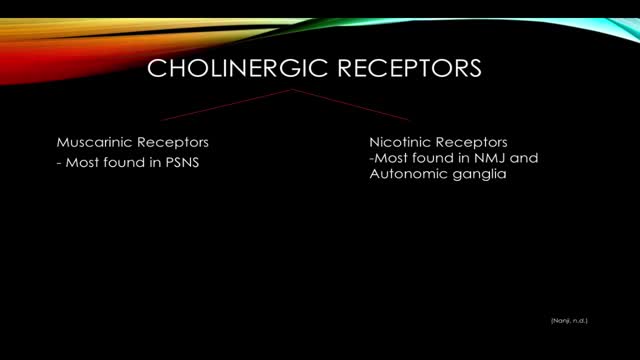
Organophosphate poisoning results from exposure to organophosphates (OPs), which cause the inhibition of acetylcholinesterase (AChE), leading to the accumulation of acetylcholine (ACh) in the body. Organophosphate poisoning most commonly results from exposure to insecticides or nerve agents.

open multi puncture testicular biopsy to retrieve sperm for ICSI (IntaCytoplasmic Sperm Injection) Procedure video

Amniocentesis,before the actual procedure, a local anesthetic is sometimes given to relieve the pain when inserting the needle used to withdraw the fluid. A needle is usually inserted through the mother's abdominal wall or at the end of the vagina, and through the wall of the uterus into the amniotic sac. With assistance from ultrasound, a physician aims towards an area of the sac that is away from the fetus and extracts a small amount of amniotic fluid for testing. The puncture heals, and the amniotic sac replenishes the liquid over a day or so. After the amniotic fluid is extracted, the fetal cells are separated from it using a centrifuge, and the fetal chromosomes are examined for abnormalities. Various genetic testing may be performed, but the three most common abnormalities tested for are Down's syndrome, Trisomy 18 and spina bifida. Amniocentesis can be performed as soon as sufficient amniotic fluid surrounds the fetus to allow a sample to be recovered relatively safely, usually no earlier than the 14th week of pregnancy. Often, genetic counseling is offered in conjunction with amniocentesis.

popliteal embolectomy; medial approach using a 4 f fogarty catheter

A subdural hematoma is a collection of blood outside the brain. Subdural hematomas are usually caused by severe head injuries. The bleeding and increased pressure on the brain from a subdural hematoma can be life-threatening.
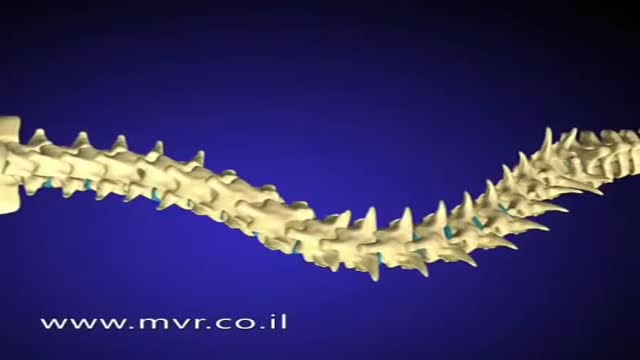
There are several approaches to scoliosis surgery, but all use modern instrumentation systems in which hooks and screws are applied to the spine to anchor long rods. The rods are then used to reduce and hold the spine while bone that is added fuses together with existing bone.

Many over-the-counter medications can help relieve heartburn. The options include: Antacids, which help neutralize stomach acid. Antacids may provide quick relief. But they can't heal an esophagus damaged by stomach acid. H-2-receptor antagonists (H2RAs), which can reduce stomach acid. H2RAs don't act as quickly as antacids, but may provide longer relief. Proton pump inhibitors, such as lansoprazole (Prevacid 24HR) and omeprazole (Prilosec OTC), which also can reduce stomach acid.

Indications for endovascular repair of the iliac artery are: Stenosis or (short-segment) occlusion of iliac artery (TASC type A and B, TASC C lesions are controversial) with ipsilateral lower extremity ischemia (lifestyle-limiting, progressive claudication, rest pain, gangrene). Patients with asymptomatic aneurysm greater than 4 cm in diameter. An iliac aneurysm which has also increased in size by 0.5 cm in last six months. Symptomatic iliac artery aneurysms mandate endovascular (or open) repair regardless of size. Patients with long occluded lesions/poor run-off/acute limb ischemia are poor endovascular candidates.

Ear Infection Drainage Time Lapse Video

Unique 3D technology from Olympus:
http://www.olympus-europa.com/....medical/en/medical_s
Discover the 3rd dimension of endoscopy and experience laparoscopy in a totally new dimension.
Contact us for more information:http://www.olympus-europa.com/....medical/en/medical_s
Multiple strains put your children and teens at risk of meningococcal meningitis. How-to ensure they are fully protected.
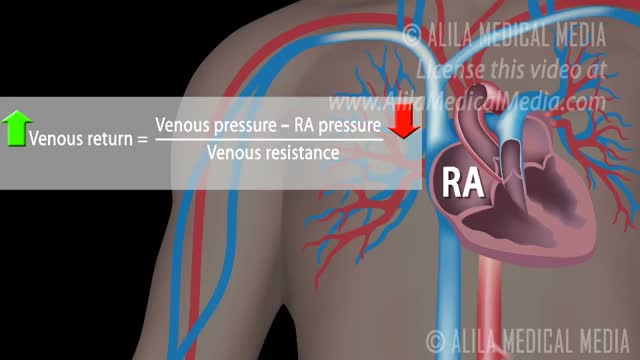
How Respiratory Pump Affects Venous Return

Whether the result of an accident or biting on a piece of food that’s too hard, mouth injuries can cause teeth to become cracked, broken, or knocked out/dislodged. It is important to see a dentist because if left untreated, a dental emergency can lead to serious complications.

Surgical Scrub How To
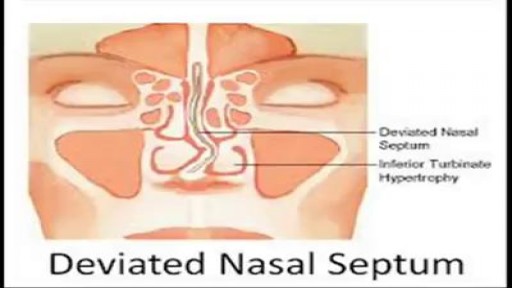
When a deviated septum is severe, it can block one side of your nose and reduce airflow, causing difficulty breathing. The additional exposure of a deviated septum to the drying effect of airflow through the nose may sometimes contribute to crusting or bleeding in certain individuals. Nasal obstruction can occur from a deviated nasal septum, from swelling of the tissues lining the nose, or from both. Treatment of nasal obstruction may include medications to reduce the swelling or nasal dilators that help open the nasal passages. To correct a deviated septum, surgery is necessar
Upper Limb Examination Video
The condition is caused by a blockage in the lymphatic system, part of the immune and circulatory systems. Lymphedema is most commonly caused by lymph node removal or damage due to cancer treatment. The main symptom is swelling in an arm or leg that may be accompanied by pain or discomfort. Exercise, wrapping, massage, and compression can help.

Watch that video to know Steroids Side Effects on The Human Body
