- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

In medicine, the caloric reflex test is a test of the vestibulo-ocular reflex that involves irrigating cold or warm water or air into the external auditory canal.

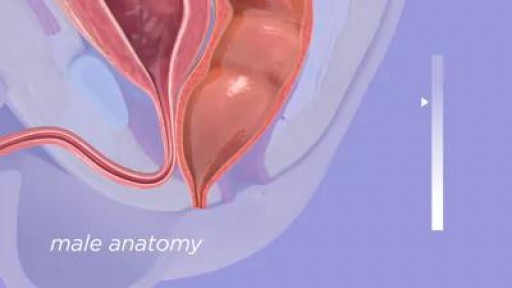
Myomectomy means the surgical removal of just the fibroid, with reconstruction and repair of the uterus. There are now a number of techniques used to perform myomectomy: through an abdominal incision, vaginal incision, with a laparoscope
Animation explaining the pancreatic auto islet transplantation process with complete removal of the pancreas to treat pancreatitis.
Buy your new Medical Marijuana Card for $59 & renewals for $45. Chat with our licensed doctors from your place and obtain your card by email in less than 10 minutes. Visit https://www.onlinemmjlosangeles.com/
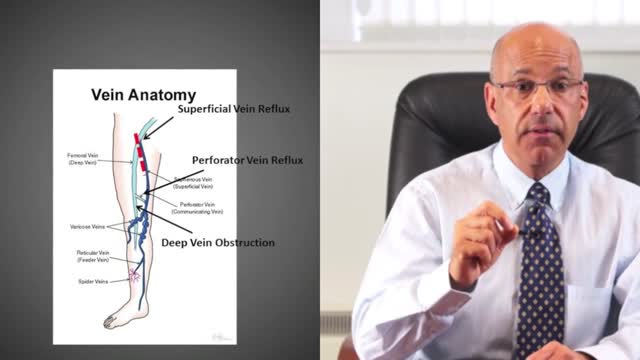
A leg ulcer is simply a break in the skin of the leg, which allows air and bacteria to get into the underlying tissue. This is usually caused by an injury, often a minor one that breaks the skin. In most people such an injury will heal up without difficulty within a week or two. However, when there is an underlying problem the skin does not heal and the area of breakdown can increase in size. This is a chronic leg ulcer.

Function and Anatomy:
Hinge type joint formed by the articulation of the Ulna and Radius (bones of the forearm), and Humerus (upper arm). Full extension is equal to 0 degrees, full flexion to ~ 150 degrees. Maximum supination (turning hand palm up so that it can hold a bowl of "soup") and pronation (palm down) are both 90 degrees


BioDigital Systems created this 3D animation of a knee replacement surgery.
---
BioDigital is happy to share helpful health information, but we do not offer medical advice. For medical advice, please contact your healthcare provider directly.
For more information on the content of this video, you can:
Access these 3D visuals: human.biodigital.com
Learn more about BioDigital: www.biodigital.com
Subscribe: www.youtube.com/c/BioDigital?sub_confirmation=1
Facebook: www.facebook.com/BioDigitalHuman
Instagram: www.instagram.com/biodigital.human
Twitter: twitter.com/biodigitalhuman
LinkedIn: www.linkedin.com/company/biodigital/ Medical disclaimer:
BioDigital, Inc is not a health care provider and we do not provide medical advice. You should not rely on the information provided on our sites or services as a substitute for, nor does it replace, professional medical advice, diagnosis, or treatment. The services are not intended to be used by consumers or clinicians in making treatment decisions. You are encouraged to seek professional medical diagnosis and treatment for any medical condition, and to discuss information from the sites and services with your healthcare provider. Information provided on the sites and media is provided for informational purposes and is in no way intended to substitute consulting a medical professional. Nothing stated or posted by BioDigital is intended to be, and must not be taken to be, the practice of medicine, the provision of medical care, or a tool relied on by patients or clinicians. If you rely on any of the information provided by BioDigital, you do so solely at your own risk.
Tooth loss can make you look older. When you lose a tooth and don’t replace it with a dental implant, you risk the chance of jawbone loss. Normally, your tooth root stimulates the continued growth and health of your jawbone. Dental implants mirror your natural tooth root and keep your jawbone healthy.

Leading cardiologists Valentin Fuster, MD, PhD, Director of Mount Sinai Heart and Herschel Sklaroff, MD, Clinical Professor of Medicine, Cardiology at Mount Sinai Heart were filmed for one-month for the “Making Rounds” documentary film as they cared for critically-ill heart patients in the Cardiac Care Unit at The Mount Sinai Hospital.
Watch Mount Sinai Heart doctors, fellows, residents, and nurses in action and saving lives demonstrating how simply listening to patients at the bedside remains medicine’s most indispensable tool over any technology.
In this film Mount Sinai Heart helps preserve the disappearing art and science of how to examine and diagnose patients at the bedside for future generations of physicians.
**This film was made possible by the generous support
of the McInerney Family.**
Copyright 2015 Middlemarch Films, Inc

how do you know if I have a clogged duct or mastitis? You'll always have a clogged duct before you have mastitis and sometimes mastitis can be prevented if you jump on it fast enough. A clogged duct may be red, it can be a tender lump on one side or the other, just feel a little bit painful in one area when you nurse, and the best thing to do is apply warm compresses especially before nursing, massage the area from your armpit down towards the nipple, and then nurse your baby. The goal is to unclog that duct, get your baby to fully empty the breast, and hopefully it will prevent an infection. An infection or mastitis develops if the clogged duct isn't unclogged and bacteria start to harbor and grow and then you have an infection. Symptoms can be the same as a clogged duct as far as how the breasts feel. You might notice a red tender area or a lump. In addition to that you usually do have a fever or flu-like symptoms or just have generalized malaise, and fatigue, and aches. If you feel this way, call your doctor as soon as possible because it requires treatment. An antibiotic is the treatment as well as drinking lots of fluids and nursing your baby as frequently as possible. The milk that comes from the clogged duct is not harmful for your baby but sometimes it tastes a little extra salty and babies refuse it. If that's the case be sure to pump so that you're emptying your breast frequently. The more frequently you empty your breast the quicker you'll get over the infection. Also, of course, taking the antibiotics your doctor has prescribed and be sure to finish the entire course. If you have any other questions for me in the future feel free to ask them on our Facebook page at Facebook.com/IntermountainMoms and recommend us to your friends and family too.
Anorectal malformations are defects that occur during the fifth to seventh weeks of fetal development. With these defects, the anus (opening at the end of the large intestine through which stool passes) and the rectum (area of the large intestine just above the anus) do not develop properly

Marfan syndrome is a genetic disorder that affects the body's connective tissue. Connective tissue holds all the body's cells, organs and tissue together. It also plays an important role in helping the body grow and develop properly. Connective tissue is made up of proteins.

Vaginal Yeast Infection

Warning! Do not watch if you are squeamish! SHOW MORE
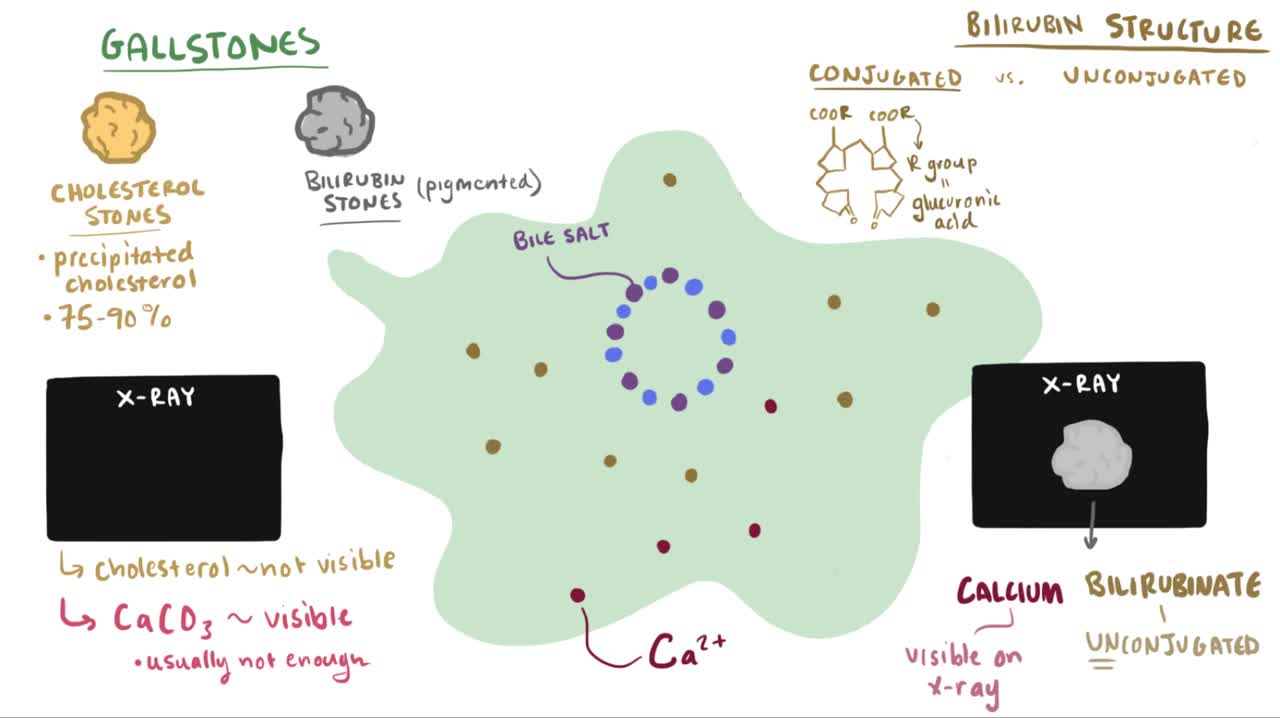
Cholelithiasis involves the presence of gallstones (see the image below), which are concretions that form in the biliary tract, usually in the gallbladder. Choledocholithiasis refers to the presence of 1 or more gallstones in the common bile duct (CBD).
Atrial flutter is a type of abnormal heart rate, or arrhythmia. It occurs when the upper chambers of your heart beat too fast. When the chambers in the top of your heart (atria) beat faster than the bottom ones (ventricles), it complicates your heart rhythm

How are seizures and epilepsy treated? What should I do if someone has a seizure? When seizure medications don't work, what else can be tried? These are just a few of the questions that you'll find answered here. Some treatment goals are common to everyone. Everyone should know what to do when a person is having a seizure. All people with seizures and their families should know that the real goal of treating epilepsy is to stop seizures or control them as best as possible. But you are more than just a seizure and how epilepsy affects you and your family may be different from someone else. Don't forget the most important goal of the Epilepsy Foundation - helping people with seizures and their families lead full and unrestricted lives according to their own wishes. Patient and doctor discussing treatment options"No seizures, no side effects" is the motto for epilepsy treatment. Not every person will reach that goal right now, but research and getting the "right care at the right time" can help more people achieve it each year. You may learn things here that can help you right away or later on. While seizure medicines are the mainstay of epilepsy treatment, there are other approaches to think about too. We hope these sections will help you learn about different treatments and get the help you need. Learn about the basics of Treatment 101 to help you get started. Look at Receiving Quality Care to see what to expect when you have just been diagnosed or after you have already started treatment. Then learn about specific treatments, what to do if seizures don't stop, and how to develop your health care team. You'll also find tools to help you manage your epilepsy or learn about research studies in other sections, so don't stop here!
As the liver becomes more severely damaged, more obvious and serious symptoms can develop, such as: yellowing of the skin and whites of the eyes (jaundice) swelling in the legs, ankles and feet, due to a build-up of fluid (oedema) swelling in your abdomen, due to a build-up of fluid known as ascites.

This is a demonstration of the Kocher's method of relocating a dislocated shoulder
