- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
USMLE Step 2 CS - LGIB This is just preview video. To get full access please visit our website : www.usmletutoring.com
Aplastic anemia is a hematopoietic disorder caused due to T lymphocyte mediated destruction of stem cells resulting in pancytopenia with a cellular bone marrow and normal cell cytogenetics. The causes of aplastic anaemia may be inherited or acquired. The causes and the diagnostic approach, along with spectrum of severity of this disorder is discussed in this presentation. A detailed discussion of the management options, along with pharmacological therapy and supportive therapy in these cases is also discussed. The treatment options include, in addition to a stem cell transplant, anti-thymocyte globulin, cyclosporine, methyprednisolone and eltrombopag (for patients who have failed treatment on combined modality therapy with ATG and cyclosporine)
USMLE Step 2 CS - Palpitations This is just preview video. To get full access please visit our website : www.usmletutoring.com
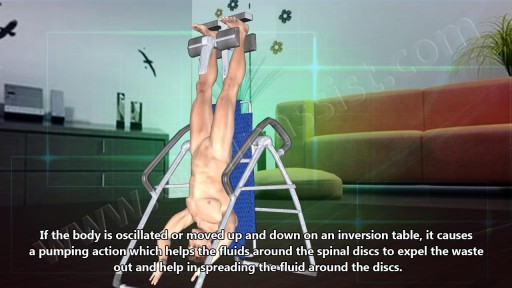
Many people report that inversion table therapy is a great way to stretch muscles and ligaments, reduce muscle spasms, and improve circulation. Stretching stimulates the lymph glands to increase the flow of lymphatic fluids; part of the body's waste disposal system. Similarly, cellular health depends on good blood circulation to deliver nourishment and remove waste. Inversion table therapy also helps to relieve motion sickness and stress. In addition, the body becomes more aware of its spatial orientation and balance when the inner ear is stimulated during inversion. Plus, it is not necessary for the body to be positioned completely upside down to gain benefits from inversion therapy! Unlike antigravity boots used with an inversion rack, an adjustable inversion table offers the flexibility to choose the most comfortable angle. Dialogue with Your Doctor Like anything that can affect your health, talk to your doctor before you start using an inversion table. This is important because certain medications and health conditions may make using an inversion table unsafe. Your doctor may recommend against inversion table therapy if you have obesity, a detached retina, fracture, glaucoma, heart condition (circulatory problem), hernia, implanted device, middle ear or eye infection, osteoporosis, are pregnant, or have a spinal injury. There may be other medical conditions not listed that your doctor may view as a contraindication.

Common causes of the knee pain
Knee pain is very common and in this video we will present the most common problems that can cause pain in the knee. (Patella) itself, which is in front of the knee, or from the tendons that are attached to the kneecap (patellar tendon and quadricep tendon). One of the most common problems is patellar chondromalacia which is chronic pain due to the softening of the cartilage beneath the kneecap. The cartilage of the kneecap will have some erosions, defects, or holes from mild to complete inside the joint (exactly in the back of the kneecap).
• Pain in the front of the knee
• Occurs more in young people
• Becomes worse from climbing up stairs and going downstairs
Treatment is usually nonsteroidal anti-inflammatory medication, physical therapy, and surgery is very rare. Also in front of the kneecap, the patient may get pain due to prepatellar bursitis.
When there is prepatellar bursitis, the patient will see that the swelling, the inflammation, and the pain is located over the front of the kneecap. The bursa becomes inflamed and fills with fluid at the top of the knee, causing pain, swelling, tenderness and a lump in that area on top of the kneecap. If the pain is in front of the knee but below or above the patella, this may indicate that the patient has tendonitis. Patellar tendonitis is an overuse condition that often occurs in athletes who perform repetitive jumping activities. Patellar tendonitis is a knee pain that is associated with focal patellar tendon tenderness and it is usually activity related. It is located below the kneecap and is called "jumper's knee". Patellar tendonitis affects approximately 20% of jumping athletes. There will be tenderness to palpation at the distal pole of the patella in extension and not in flexion. Quadriceps inflexibility, atrophy and hamstring tightness are predisposing factors for this condition. Treatment is rest, anti-inflammatory medication, stretching and strengthening of the hamstrings and quadriceps. Use an eccentric exercise program. The early stages of patellar tendonitis will respond well to nonoperative treatment. Another important cause of knee pain is a meniscal tear. The meniscus is the cushion that protects the cartilage in the knee. Injury will cause pain on the medial or the lateral side of the knee exactly at the level of the joint. The patient will complain of a history of locking, instability and swelling of the knee. McMurray test will be positive. A painful pop or click is obtained as the knee is brought from flexion to extension with either internal or external rotation of the knee. Arthritis of the knee Knee arthritis is very common. The cartilage cells die with age and its repair response decreases in the joint collapses with increased breakdown of the framework of the cartilage. The patient will have progressive blurring away of the cartilage of the joint with decreased joint space as seen on x-rays. Another source of pain is the Baker's cyst. The cyst is in the back of the knee between the semimembranosus yes and the medial gastrocnemius muscles. Another important source of knee pain is a ligament injury. Here is a normal knee without a ligament injury. Here you can see from the front, you can see the lateral and medial collateral ligament. You can see the ACL and PCL from the side view. These ligaments are usually injured as a result of a sports activity. Here is an example of a sports knee injury. Here is an example of the medial collateral ligament injury. This is the most commonly injury knee ligament injury to this ligament is on the inner part of the knee. Here is an example of an injury of the anterior cruciate ligament. It involves a valgus stress to the knee. Lachman test is usually positive, and MRI is diagnostic. Another important cause of knee pain is iliotibial band syndrome of the knee. Inflammation of the thickening of the iliotibial band results from excessive friction as the iliotibial band slides over the lateral femoral condyle. The iliotibial band is a thick band of fascia that extends along the lateral thigh from the iliac crest to the knee. And as the knee moves, the IT band was repeatedly shifted forwards and backwards across the lateral femoral condyle. The patient will complain of swelling, tenderness, and crepitus over the lateral femoral condyle. The condition occurs in the ITB S occurs in runners, cyclist and athletes that require repeated knee flexion and extension. The pain may be reproduced by doing a single-leg squat. The Ober's test is used to at assess tightness of the iliotibial band. MRI may show edema in the area of the ITB. Treatment is usually nonoperative with rest and ice, physical therapy, with stretching, proprioception, and improvement in neuromuscular coordination. Training modification and injections may be helpful. Surgery is a last resort. Surgical excision of the scarred inflamed part of the iliotibial band.
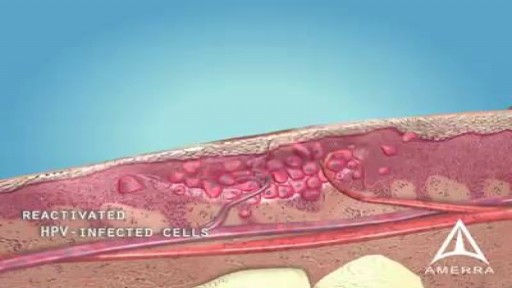
A wart is a skin growth caused by some types of the virus called the human papillomavirus (HPV). HPV infects the top layer of skin, usually entering the body in an area of broken skin. The virus causes the top layer of skin to grow rapidly, forming a wart. Most warts go away on their own within months or years.
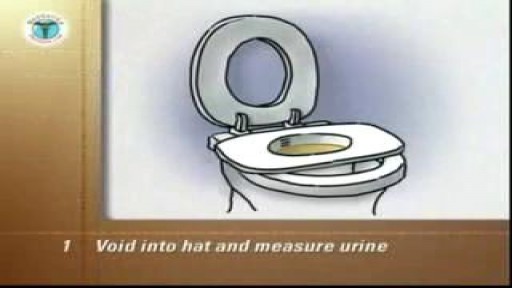
Female Intermittent Self Catheterization

Hirschsprung's (HIRSH-sproongz) disease is a condition that affects the large intestine (colon) and causes problems with passing stool. The condition is present at birth (congenital) as a result of missing nerve cells in the muscles of the baby's colon. A newborn who has Hirschsprung's disease usually can't have a bowel movement in the days after birth. In mild cases, the condition might not be detected until later in childhood. Uncommonly, Hirschsprung's disease is first diagnosed in adults.

Watch that video to know How to Stop Arterial Bleeding

Myomectomy means the surgical removal of just the fibroid, with reconstruction and repair of the uterus. There are now a number of techniques used to perform myomectomy: through an abdominal incision, vaginal incision, with a laparoscope

A displaced fibular head can create tightness, pain, and even numbness or tingling along the outside of your knee and down your leg. This most often occurs after a modest hyperextension knee injury, such as landing on one leg after jumping. If you have lingering knee pain and are searching for an answer, try this move

Bandaging a freshly above the knee amputated limb

Watch that video to know the Types of Female Genital Infection Yeast or Candidiasis, Trichomoniasis, Bacterial Vaginosis


A new well designed randomized study has suggested that long term baby aspirin usage may aid in fight against cancer. The suggested mechanism is that cancers induce inflammatory responses so the anti-inflammatory mechanism of prostaglandins inhibitors may cease the progress of many cancers. There are some concerns about the study because despite the well-designed randomized study; the study didn't include a satisfying number of female participants. The study was also conducted on esophageal, colorectal and lung cancers.
Vital Signs and Chest Examination
Best facial cosmetic surgeons Best facial plastic surgeon
Borderline Personality Disorder Information

Excision of Rectovaginal Nodule
