- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
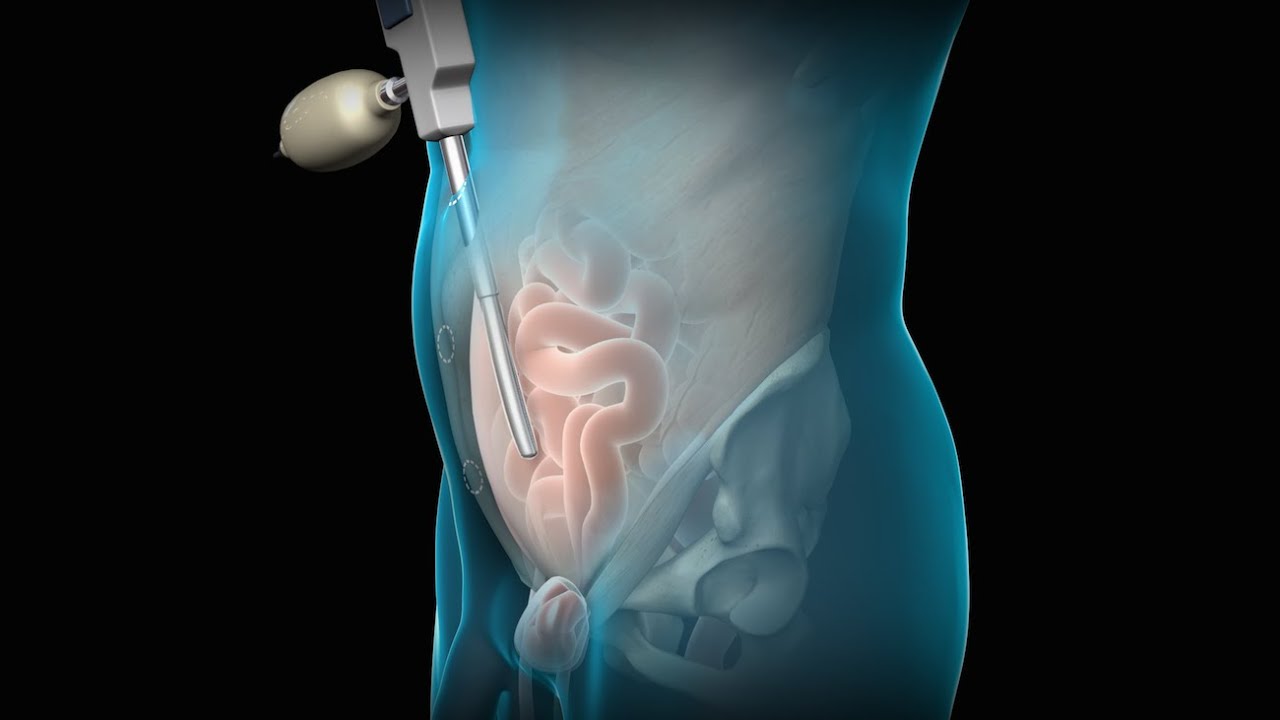
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
















Anterior Elevate Mesh Repair performed by Dr. Robert Moore and Dr. John Miklos
Anterior vaginal wall relaxation (cystocele) is one of the most commonly diagnosed forms of pelvic organ prolapse in women. More than 200,000 cystocele repairs are completed yearly, however to date the procedures that are completed do not provide very high cure rates and/or poor anatomic outcomes. Successful treatment of anterior vaginal wall prolapse remains one of the most challenging aspects of pelvic reconstructive surgery we face. We have developed very good procedures that provide excellent support for the posterior wall (ie rectoceles) and the apex of the vagina (ie vaginal vault prolapse) and reproduce normal anatomy. We were one of the first centers in the country to utilize grafts in rectocele repairs and have seen improved cure rates to over 90% with minimal complications. It has been known for many years that abdominal sacralcolpopexy with placement of a mesh graft at the top of the vagina for vaginal vault prolapse is the most successful procedure in the literature. We have made advancements with this procedure as well in being able to offer our patients a laparoscopic minimally invasive approach for sacralcolpopexy, with the same excellent cure rates (>92%) and with hospital stays typically less than 24 hours and reduced complications. However the anterior wall has been one of the most difficult compartments in the vagina to get good anatomic results and high cure rates with traditional repairs and at the same time not cause sexual dysfunction, pain with intercourse, voiding dysfunction (ie incontinence or urgency/frequency syndrome), or a shortened or scarred down vagina. The transobturator approach was developed as a less invasive way to place an anterior wall graft (see below) however this still involved blind needle passes and the graft did not support the apex of the vagina, therefore the search for improvements in these procedures is ongoing.
