- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other

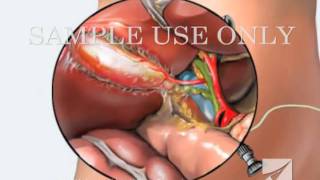
















Removal of multiple stomach tumors
ENDOSCOPIC (NON-SURGICAL) REMOVAL OF MULTIPLE LARGE TUMORS FROM STOMACH IN A PATIENT WITH PEUTZ-JEGHERS SYNDROME
PEUTZ-JEGHERS SYNDROME: Peutz-Jeghers syndrome (PJS) is a familial syndrome consisting of mucocutaneous pigmentation, gastrointestinal polyposis and cancers of gut & other sites like breast, ovary, and testes. PJS has an autosomal dominant inheritance with variable and incomplete penetrance. Germline mutations of STK11/LKB1 gene on 19p cause this syndrome. Mucocutaneous pigmentation may be noted in early infancy. These deposits of melanin are most commonly found around the mouth, nose, lips, buccal mucosa, hands, and feet, and may also be present in perianal and genital areas. PJS polyps may be found in stomach, small intestine, or colon, but they tend to be prominent in the small intestine. These polyps may increase in size and cause small intestinal obstruction or intussusceptions that may occur in early infancy. Acute upper gastrointestinal bleeding and chronic faecal blood may complicate the disease.
PATIENT: The patient was a 25 yr male who had mucocutaneous pigmentation and multiple polyps in the stomach and duodenum. He presented with bleeding from gastric polyps. As the polyps in stomach were numerous, (more than 20 in number) and were large in size (some equal to small egg size), he had been advised to undergo surgery. Surgery planned was total gastrectomy.
PROCEDURE: The patient underwent video-endoscopy of the esophagus, stomach and duodenum. All polyps were examined for size and presence or absence of stalk. A plan to remove all the gastric polyps at endoscopy was made in the same sitting. He received light conscious sedation. Flat polyps were raised form the gastric wall by injection of saline in to polyp base to let these lesions have a stalk. This was done by needle injector. Each polyp was engaged in a snare and the polyp stalk was cut by coagulation cutting current. The cuts were clean without any bleeding. All polyps were recovered for histology. The histology revealed all polyps to be hamartomous lesions. None of the polyps were cancerous. Patient has been followed up for over one year and is doing fine without any further bleeding or pain.
Video shows the procedure of videoendoscpy and endoscopic removal of polyps.

SORT BY-
Top Comments
-
Latest comments